The front desk phone is the first, and often the most frustrating, touchpoint a patient has with your clinic. Long hold times, missed calls during lunch coverage, and after-hours voicemail black holes push patients to reschedule elsewhere or simply not book at all. AI voice agents are increasingly filling that gap, handling scheduling, reminders, insurance questions, and routine follow-up so front-desk staff can focus on the patients standing in front of them. This guide covers how clinics are actually using AI voice agents in 2026, and where the technology should stop and a human should take over.
Administrative friction is one of the most persistent problems in outpatient care. Patients frequently report sitting on hold for twenty to thirty minutes navigating phone menus just to book or change an appointment, and industry-wide estimates from the CAQH Index put the cost of manual, non-digitized administrative processes across U.S. healthcare at roughly $12.6 billion a year in unnecessary spend. Physicians, meanwhile, are buried in prior authorization work: AMA survey data shows the average physician completes 39 to 45 prior authorizations a week, consuming about 12 hours of staff time in the process.
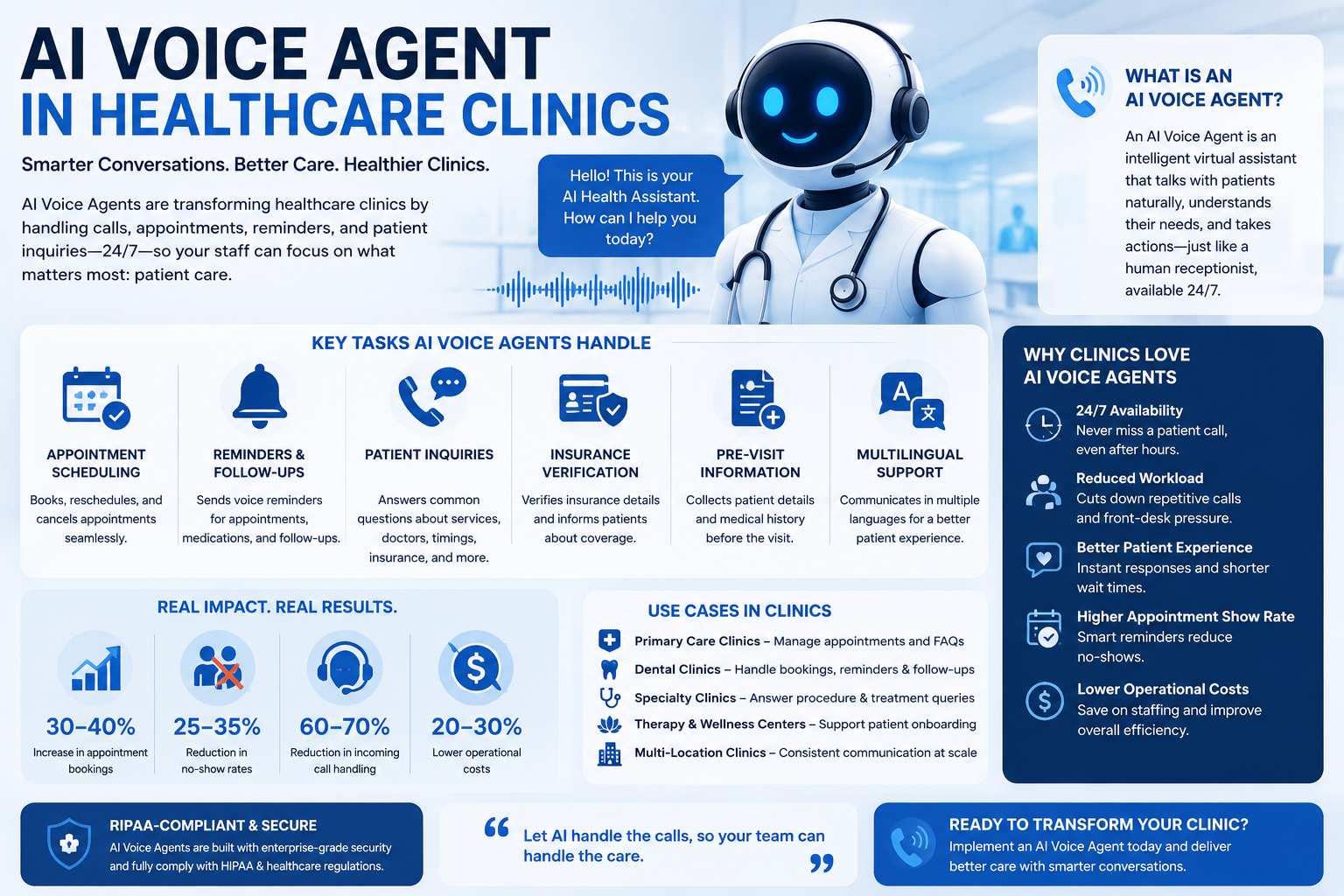
AI voice agents aren’t a fix for clinical decision-making, and no reputable deployment treats them that way. What they are proving effective at is absorbing the repetitive, rules-based phone work that eats staff time and frustrates patients: scheduling, reminders, insurance verification calls, and routine follow-up, with a clear, non-negotiable handoff to a human whenever a call touches anything clinical.
Two forces are converging to make this a practical option rather than an experimental one: patient expectations for immediate access have risen, and voice AI has matured enough to handle real scheduling and EHR-connected workflows rather than simple menu-style call routing.
Vendor-reported case studies illustrate the scale of the opportunity, while still warranting the same scrutiny any vendor claim deserves. One widely cited healthcare deployment reported a 91% call automation rate with zero call abandonment during a demand surge, and another practice-management rollout reported an 86% reduction in call volume reaching staff along with a 40% drop in no-shows. These are results reported by the vendors involved rather than independently audited figures, so treat them as a directional signal of what’s achievable with a well-run deployment, not a guarantee.
| Use case | What the agent handles | Why it matters |
|---|---|---|
| Appointment scheduling | Booking, rescheduling, and cancellations against real-time provider availability | Captures after-hours demand and eliminates hold-time abandonment |
| Appointment reminders | Automated outbound calls or confirmations ahead of a visit | Directly reduces no-show rates, one of the most consistent reported outcomes |
| Insurance verification | Collecting and confirming coverage details before a visit | Reduces front-desk time spent on hold with payers |
| Prescription refill requests | Intake of refill requests for routing to clinical staff for approval | Removes a high-volume, low-complexity call type from the phone queue |
| Post-visit follow-up | Check-in calls, satisfaction surveys, and preventive screening outreach | Improves follow-up completion without adding staff hours |
| Billing questions | Routine balance and billing inquiries | Frees billing staff for calls that genuinely need a person |
Appointment scheduling and reminder calls are the most common starting point because they’re high-volume, rules-based, and directly tied to a measurable outcome like no-show rate. Prove value there before expanding into insurance verification or billing.
Define exactly which words, symptoms, or requests trigger an immediate handoff to a human clinician or an instruction to call 911, before the agent ever takes a live call. This is the single most important design decision in a healthcare voice deployment, not an afterthought to add later.
Any vendor handling protected health information over the phone needs to sign a Business Associate Agreement and be able to describe, specifically, how they encrypt data in transit and at rest, control access, and log activity for audit purposes. If a vendor is vague on any of these points, that’s a reason to keep looking.
A voice agent that can’t see real appointment availability or write back to your practice management system creates double-entry work instead of removing it. Integration depth, not conversational polish, is usually the difference between a tool staff trust and one they route around.
Run the agent on one workflow, such as reminder calls, for a defined period and measure it against a clear baseline. A successful pilot builds staff and patient trust before you expand into more sensitive workflows like insurance verification.
Call abandonment rate, no-show rate, average hold time, and staff hours reclaimed are more useful indicators of success than raw call volume handled. Review these weekly during the pilot and monthly once the agent is in steady-state use.
An AI voice agent in a clinic setting should be scoped to administrative and operational tasks: scheduling, reminders, verification, and routine follow-up. It should never be positioned to a patient as a source of medical advice or a substitute for clinical judgment.
Every credible healthcare voice deployment includes a risk-tier framework and a hard-coded escalation rule: if a caller mentions a red-flag symptom, such as chest pain or difficulty breathing, or otherwise indicates a possible emergency, the system immediately transfers the call to a human clinician or instructs the caller to hang up and dial 911. This human-in-the-loop safeguard is treated as a baseline requirement across the industry, not an optional feature, and clinics should confirm exactly how a prospective vendor implements it before signing a contract.
High Dreams LLC designs and deploys custom AI voice agents built around the specific workflow a business needs automated, from call routing and scheduling logic to CRM and system integrations. For a clinic, that means the agent is scoped narrowly to administrative tasks like scheduling and reminders, built with clear escalation rules from day one, and connected to the systems your front desk already uses.
Because healthcare deployments carry specific regulatory requirements, any clinic evaluating a voice agent, whether built by High Dreams LLC or another provider, should confirm the vendor’s specific HIPAA compliance posture, BAA terms, and escalation protocol directly with their team before rolling out a solution that touches patient calls. That conversation should happen before the contract, not after.
Book a free consultation with High Dreams LLC to scope a pilot around your highest-friction call type, appointment scheduling, reminders, or intake, and get a clear plan for escalation and compliance requirements.
No. AI voice agents used in clinics should be scoped to administrative tasks like scheduling, reminders, and insurance verification. They should never be presented as a source of medical advice, and any call involving symptoms or clinical questions should be escalated to a human.
No. HIPAA compliance depends on how the specific platform is built and deployed, not on the technology category. It requires a signed Business Associate Agreement, encryption in transit and at rest, access controls, and audit logging. Clinics should verify these directly with any vendor rather than assuming compliance.
A properly designed system includes a hard-coded escalation rule that immediately transfers the call to a human clinician or instructs the caller to hang up and dial 911 when red-flag symptoms or emergency language are detected. This safeguard should be verified and tested before a system goes live, not assumed.
Appointment scheduling and reminder calls are typically the best starting point. They’re high-volume, rules-based, and tied to a clear, measurable outcome, reduced no-shows, which makes it easier to prove value before expanding into more sensitive workflows.
Yes, transparency is considered a baseline best practice and, in a growing number of jurisdictions, a legal requirement. Clinics should disclose clearly at the start of the call that the patient is speaking with an AI system.
AI voice agents work well in clinics when they’re scoped tightly to administrative tasks, scheduling, reminders, insurance verification, and routine follow-up, and paired with a strict, tested escalation protocol for anything clinical. The clinics seeing real results aren’t asking AI to replace judgment; they’re using it to absorb the repetitive phone work that keeps patients on hold and staff away from the people in front of them. Start with one call type, confirm compliance in writing, and build the safety net before you build anything else.

AI Chatbot for Educational Instituation - highdreamsllc.com
July 13, 2026 at 6:12 am
“ […] AI Agents for Lead Generation: A Complete Guide to Autonomous Growth Systems in 2026Read more → AI Voice Agent in Healthcare ClinicsRead more → Why Businesses Are Investing in AI Customer SupportRead more […] “
AI Voice Agents Increase Appointment Bookings
July 13, 2026 at 12:54 pm
“ […] in Growing Your BusinessRead more → Best Industries Using AI Voice Agents in 2026Read more → AI Voice Agent in Healthcare ClinicsRead more → How AI Voice Agents Improve Amazon Online Business in 2026Read more […] “